

Where does GIST occur?
Is GIST very common?
What causes GIST?
Who gets GIST?
What symptoms can indicate GIST?
Hyperlinked terms are defined in the glossary section of this website. Click the term to see a pop-up definition.
Gastrointestinal stromal tumor (GIST) is a rare cancer affecting the digestive tract or nearby structures within the abdomen. GI stromal tumor, or GIST cancer, is a sarcoma. Sarcomas are cancers that grow from cells of the body’s connective or supportive tissues such as bone, cartilage, tendons, nerves, fat, muscle, synovial tissue (tissue around joints), or blood vessels. (Most cancers are carcinomas, not sarcomas.)
GIST cancers arise either from cells called Interstitial Cells of Cajal (ICCs) or from less differentiated stem cells or precursor cells that can develop into ICCs. The ICCs are known as “pacemaker cells of the gut” because they send signals to trigger peristalsis, the digestive tract’s muscular contractions that move food along its course.
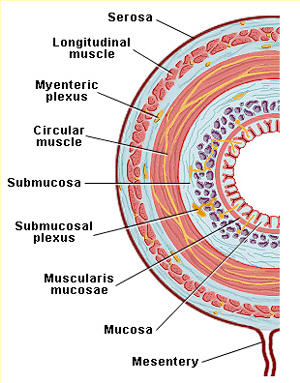 |
| Layers of the Gastrointestinal Tract. Figure from Section VI, Gastrointestinal Physiology (Ginsburg, J.M. and Costoff, A.) in Essentials of Human Physiology (edited by Nosek, T.M.), reproduced with kind permission of the copyright holder, The Medical College of Georgia. |
In the diagram at right you can see the circular and longitudinal muscle layers of the GI tract, with the myenteric plexus layer between the two muscle layers. The ICCs are found in the wall of the gastrointestinal (GI) tract between the GI tract’s muscular layers. They are not related to the cells that line the inside of the tract’s lumen (the hollow tube of the food passageway, shown as the “doughnut hole” in the diagram). The cells lining the lumen form the so-called gastrointestinal epithelium (mucosa) and give rise to the more common forms of gastric, intestinal, and colon cancer.
Because GIST cancers arise from the GI tract wall, they are usually attached to the outside of the involved organ, growing outward; this is sometimes referred to as exophytic. Occasionally a GIST may grow inward through the muscle layer of the GI tract wall and then develop partly inside the digestive tract lumen; this is sometimes called endophytic.
Where does GIST occur?
Primary tumors are in the original site of development, before any spread to other locations. Primary gastrointestinal stromal tumors (GIST cancers) may occur anywhere along the gastrointestinal tract from the esophagus to the anus.
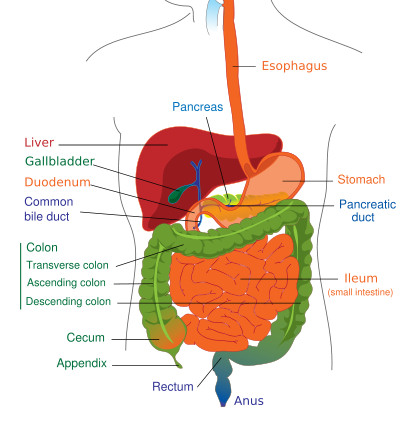 The most frequent site for GISTs is the stomach (about 55%), followed by the duodenum and small intestine (about 30%), esophagus (about 5%), rectum (about 5%), colon (about 2%), and rare other locations.
The most frequent site for GISTs is the stomach (about 55%), followed by the duodenum and small intestine (about 30%), esophagus (about 5%), rectum (about 5%), colon (about 2%), and rare other locations.
Occasionally, primary GISTs may develop in the supporting membranes of the abdominal organs (peritoneum, mesentery, omentum), the liver, the pancreas, the ovaries, the uterus, and the prostate. Because primary GISTs in these locations do not arise directly from the GI tract, they are sometimes called “extragastrointestinal” stromal tumors (Reith et al, 2000). When a GIST grows in a location where it is not encased in the peritoneal membranes, it is said to be retroperitoneal. For example, GISTs attached to some sections of the duodenum are retroperitoneal.
Cancer is most threatening when it metastasizes or spreads to additional locations beyond the primary tumor site. In GIST the most common sites for metastasis are the liver and the abdominal membranes (peritoneum, mesentery, omentum). GIST rarely spreads to lymph nodes, but it may occasionally affect local abdominal lymph nodes. Unusual sites of metastasis include lung and bone tissue, as well as pelvic sites such as the ovaries (Belics et al, 2003; Irving et al, 2005; Wingen et al, 2005). Extremely rare sites of metastasis include breast (Igwilo et al, 2003) and muscle tissue.
![]()
References are included in case you want to know where to find more information. All the references are listed in the Further Reading and References page, including the PubMed ID for each one. Click the title of the reference to see its listing in PubMed, where you can read the abstract of the article and see its source.
Is GIST very common?
Gastrointestinal stromal tumor (GIST) is quite rare. Most cancers are carcinomas, meaning that they derive from cells in the skin (or epithelium), either our outer-body skin or the skin-like lining of our internal body cavities and the digestive or gastrointestinal (GI) tract. Most GI tract cancers are carcinomas, such as those commonly known as stomach cancer, colon cancer, etc. GIST is not related to these common GI cancers; it is a sarcoma. Of all adult cancers, sarcomas represent about 1%. GIST is one of the more common of about 50 t
ypes of sarcoma. To get some perspective, there are about 1.4 million new cases of cancer per year in the USA (Jemal et al, 2004), and only about 15,000 of these are sarcomas (Borden et al, 2003).
One careful retrospective study of all GI tumor samples for a region in Sweden identified a yearly incidence of 13.8 KIT-positive GISTs per million people (Nilsson et al, 2005). If the same incidence were applicable in the USA, there would be about 4000 GISTs per year in America. In contrast, a study based on cases of GIST reported to SEER cancer registries in the USA estimated a much lower incidence of 6.8 per million (Tran et al, 2005). However, because many cases have been misdiagnosed or not reported, and the SEER data included only those tumors judged to be malignant, this estimate is bound to be too low. Another recent estimate from Norway is higher: 19.9 cases per million in Norway in 1994-2003 (Steigen and Eide, 2006). The available population-based estimates (which count all cases in a defined region over time) are compared in the following table.
|
Annual Incidence of GIST in Population-Based Studies |
||
| Study and Location | Crude Incidence | Age-Adjusted Incidence |
| Nilsson et al (2005) western Sweden |
14.5 per million | |
| Tryggason et al (2005) Iceland |
11.1 per million | |
| Goettsch et al (2005) Netherlands |
12.7 per million | |
| Rubió et al (2007) region of Spain |
9 per million | |
| Mucciarini et al (2007) region of Italy |
14.2 per million | 6.6 per million |
| Mazzola et al (2008) region of Switzerland |
19.6 per million | 14.7 per million |
| Yan et al (2008) region of Canada |
9.1 per million | |
| Ducimetière et al (2011) region of France |
11.1 per million | 9.0 per million |
It is often stated that gastrointestinal stromal tumors are the most common mesenchymal tumors of the GI tract, but this only means that they are slightly less rare than the other tumors in this category. GISTs account for only 1-3% of gastric (stomach) tumors, about 20% of small bowel tumors, and 1% or less of colorectal tumors. The vast majority of tumors in these locations are carcinomas within the tissues lining the GI tract. Most primary care physicians and many pathologists and oncologists go through their entire professional careers without seeing a single GIST. This is important to patients because misdiagnosis can delay the start of appropriate treatment. The physicians at major cancer referral treatment centers, especially those with sarcoma teams, are much more likely to be familiar with gastrointestinal stromal tumor and its treatment.
![]()
What causes GIST?
There are no known environmental or behavioral risk factors contributing to GIST. Therefore, patients should not worry that their diet or lifestyle choices contributed to GIST. Random genetic mutations are the apparent cause of GISTs. The majority of GISTs show identified mutations in cell-surface proteins called tyrosine kinase receptors. These mutations are discussed further in the pages on Diagnosis and Pathology Results as well as Mutation Analysis. Most GISTs show mutations in a gene that produces a growth factor receptor called KIT. A few GISTs show mutations in the gene for a closely related receptor for platelet derived growth factor receptor alpha (PDGFR a or PDGFRA). A few GISTs are normal or “wildtype” for both these genes, and the causal mutations or these GISTs have not been identified. Almost all GISTs are sporadic, meaning that the mutations are random occurrences affecting a single individual. However, there are rare examples of GIST running in families due to an inheritable germline mutation (see Familial GIST page). In addition, people affected by neurofibromatosis type 1 (NF1) have an increased chance of developing GIST (see our page GIST in NF1).
![]()
Who gets GIST?
Like most other cancers, GIST most commonly affects older people, usually over age of 50 years. The median age at which sporadic GIST is found is about 60 years old. Children are affected very rarely (see pages on Pediatric GIST and Carney Triad). Persons with inactivation of the neurofibromatosis 1 gene (NF1) are more likely to develop GIST than the general population (see page on GIST in NF1) and are more likely to be diagnosed at younger ages. Familial GIST also develops in younger or middle-aged adults (see page on Familial GIST). GIST is found in populations around the world. There is no good information about whether its incidence is more common in certain racial or ethnic groups.
![]()
What symptoms can indicate GIST?
Many patients (mostly those with smaller tumors) have no symptoms. Larger tumors may cause symptoms that are generally related to the increased mass being accommodated in the abdominal cavity, and such symptoms would not necessarily be different from those other types of tumors. These symptoms include digestive discomfort, sensations of abdominal fullness, or abdominal pain. Sometimes larger tumors may be detectable as a mass when feeling the abdomen, or as a visible enlargement of the abdomen. Some patients experience vomiting or diarrhea. Bowel obstruction may occur. Sometimes GISTs perforate the stomach or gut lining and bleed into the GI tract, resulting in black or tarry stools, or occasionally in vomiting of blood. Anemia may result from chronic bleeding, leading to fatigue. Sometimes anemia may cause the patient’s heart to race (tachycardia). The patient may notice weight loss. Very rarely a GIST may rupture, making its presence known with a medical emergency.
Though such symptoms are possible, most of them are rather indistinct and merely related to the additional mass that is present in the abdomen. Therefore, many GISTs are found incidentally through medical imaging for other purposes or through surgery for other conditions. For example, in Japan endoscopic screening is done to detect carcinoma of the stomach; therefore, gastric GISTs are often found at an earlier stage in Japan because their influ
ence on the stomach lining can be seen with the endoscope.
REFERENCES
Belics Z, Csapo Z, Szabo I, Papay J, Szabo J, Papp Z.
Large gastrointestinal stromal tumor presenting as an ovarian tumor. A case report.
J Reprod Med. 2003 Aug;48(8):655-8. PMID: 12971151
Borden EC, Baker LH, Bell RS, Bramwell V, Demetri GD, Eisenberg BL, Fletcher CD, Fletcher JA, Ladanyi M, Meltzer P, O’Sullivan B, Parkinson DR, Pisters PW, Saxman S, Singer S, Sundaram M, van Oosterom AT, Verweij J, Waalen J, Weiss SW, Brennan MF.
Soft tissue sarcomas of adults: state of the translational science.
Clin Cancer Res. 2003 Jun;9(6):1941-56. PMID: 12796356
Ducimetière F, Lurkin A, Ranchère-Vince D, Decouvelaere AV, Péoc’h M, Istier L, Chalabreysse P, Muller C, Alberti L, Bringuier PP, Scoazec JY, Schott AM, Bergeron C, Cellier D, Blay JY, Ray-Coquard I.
Incidence of sarcoma histotypes and molecular subtypes in a prospective epidemiological study with central pathology review and molecular testing.
PLoS One. 2011;6(8):e20294. PubMed PMID: 21826194; PubMed Central PMCID:PMC3149593.
Goettsch WG, Bos SD, Breekveldt-Postma N, Casparie M, Herings RM, Hogendoorn PC.
Incidence of gastrointestinal stromal tumours is underestimated: results of a nation-wide study.
Eur J Cancer. 2005 Dec;41(18):2868-72. PMID: 16293410
Igwilo OC, Byrne MP, Nguyen KD, Atkinson J.
Malignant gastric stromal tumor: unusual metastatic patterns.
South Med J. 2003 May;96(5):512-5. PMID: 12911195
Irving JA, Lerwill MF, Young RH.
Gastrointestinal stromal tumors metastatic to the ovary: a report of five cases.
Am J Surg Pathol. 2005 Jul;29(7):920-6. PMID: 15958857
Mazzola P, Spitale A, Banfi S, Mazzucchelli L, Frattini M, Bordoni A.
Epidemiology and molecular biology of gastrointestinal stromal tumors (GISTs): a population-based study in the South of Switzerland, 1999-2005.
Histol Histopathol. 2008 Nov;23(11):1379-86. PMID: 18785120
Mucciarini C, Rossi G, Bertolini F, Valli R, Cirilli C, Rashid I, Marcheselli L, Luppi G, Federico M.
Incidence and clinicopathologic features of gastrointestinal stromal tumors. A population-based study.
BMC Cancer. 2007 Dec 20;7:230. PMID: 18096058
Nilsson B, Bümming P, Meis-Kindblom JM, Odén A, Dortok A, Gustavsson B, Sablinska K, Kindblom LG.
Gastrointestinal stromal tumors: the incidence, prevalence, clinical course, and prognostication in the preimatinib mesylate era–a population-based study in western Sweden.
Cancer. 2005 Feb 15;103(4):821-9. PMID: 15648083
Reith JD, Goldblum JR, Lyles RH, Weiss SW.
Extragastrointestinal (soft tissue) stromal tumors: an analysis of 48 cases with emphasis on histologic predictors of outcome.
Mod Pathol. 2000 May;13(5):577-85. PMID: 10824931
Rubió J, Marcos-Gragera R, Ortiz MR, Miró J, Vilardell L, Gironès J, Hernandez-Yagüe X, Codina-Cazador A, Bernadó L, Izquierdo A, Colomer R.
Population-based incidence and survival of gastrointestinal stromal tumours (GIST) in Girona, Spain.
Eur J Cancer. 2007 Jan;43(1):144-8. PMID: 17055254
Steigen SE, Eide TJ.
Trends in incidence and survival of mesenchymal neoplasm of the digestive tract within a defined population of northern Norway.
APMIS. 2006 Mar;114(3):192-200. PMID: 16643186
Tran T, Davila JA, El-Serag HB.
The epidemiology of malignant gastrointestinal stromal tumors: an analysis of 1,458 cases from 1992 to 2000.
Am J Gastroenterol. 2005 Jan;100(1):162-8. PMID: 15654796
Tryggvason G, Gislason HG, Magnusson MK, Jonasson JG.
Gastrointestinal stromal tumors in Iceland, 1990-2003: the Icelandic GIST study, a population-based incidence and pathologic risk stratification study.
Int J Cancer. 2005 Nov 1;117(2):289-93. PMID: 15900576
Tryggvason G, Kristmundsson T, Orvar K, Jónasson JG, Magnússon MK, Gíslason HG.
Clinical study on gastrointestinal stromal tumors (GIST) in Iceland, 1990-2003.
Dig Dis Sci. 2007 Sep;52(9):2249-53. PMID: 17420941
Wingen CB, Pauwels PA, Debiec-Rychter M, van Gemert WG, Vos MC.
Uterine gastrointestinal stromal tumour (GIST).
Gynecol Oncol. 2005 Jun;97(3):970-2. PMID: 15943997
Yan BM, Kaplan GG, Urbanski S, Nash CL, Beck PL.
Epidemiology of gastrointestinal stromal tumors in a defined Canadian Health Region: a population-based study.
Int J Surg Pathol. 2008 Jul;16(3):241-50.
PMID: 18573781
nbsp;