

Pathology Analyses for GIST
Although the level of detail depends upon whether the sample is a tiny biopsy or an entire surgically resected tumor, the pathologist generally follows the same basic protocol:
- To describe the type of sample and its visual appearance to the naked eye (called macroscopic description or gross description)
- To describe characteristics of the tissue when viewed under a microscope (called microscopic description)
- To perform immunohistochemical tests that detect the presence or absence of certain proteins that can identify the type of cells composing the tumor.
Gross Description
In the macroscopic or gross description section of the report, the pathologist will record the visible features of the specimen.
Extent of specimen: The tumor may have been resected with only a small wedge of the stomach attached to it, or the surgeon may have had to remove the tumor together with parts of several organs that were adhered to it. The pathologist will detail the anatomical parts of the specimen.
Origin of the tumor: The pathologist will identify the point along the GI tract from which the tumor arose. Gastric GIST is the most common, as shown in the next illustration.

Figure 3. Distribution of GIST in the various portions of the gastrointestinal tract. Less than 1 % of GISTs initially occur outside of these organs.
The "other" category includes rare sites for primary GIST. Occasionally, a GIST will develop from membranes within the abdomen (such as the omentum and mesentery) rather than being directly attached to the digestive tract itself. Very rarely, a primary GIST may develop from another organ such as the pancreas or the liver. (GIST metastases to the liver and to the abdominal membranes are common.)
For a tutorial on anatomy for GIST, see Abdominal Anatomy.
Size of tumor: The pathologist will measure the tumor’s largest dimensions and report them in centimeters. You can translate this to inches: 2.54 cm = 1 inch. A 5-cm GIST would be just less than 2 inches across, about the size of a lemon.
Other characteristics: Some other features of the tumor that may be present include the following.
- Necrosis: areas of dead tissue within the tumor resulting from tumor growth that outstrips the blood supply to interior parts as the tumor grows. Unlike other sarcomas, the presence of necrosis in GIST is not clearly linked to tumor aggressiveness.
- Cystic degeneration: over time, some GISTs may form a cavity or cyst containing fluid within the tumor.
- Invasion of or adherence to adjacent organs: the tumor may have become adherent to adjacent structures (often because of inflammation) without invasion into the other organ, or tumor cells may have invaded nearby structures by actually growing into them (uncommon for GIST). Usually GISTs have pushing borders and tumor cells do significantly infiltrate adjacent structures.
Surgical Margins
Surgeons attempt to remove a margin of normal tissue around the point of origin of the GIST to minimize the chances of cells being left behind that could grow later, causing local recurrence. In addition, the surgeon may remove sections of structures adjacent to the GIST if the tumor was adherent to them; in this case a margin of normal tissue will also be sought on the resected part of the adjacent structure. The distances to the margins are measured in the gross specimen and then all margins are examined microscopically with emphasis on the margin(s) closest to the tumor. Usually the gross and microscopic assessments are similar, but sometimes the microscopic examination reveals something not seen with the naked eye, and in this case, the microscopic margin is the assessment that is present in the final report. Margins are described using the following terminology:
- R0 resection indicates complete removal of all tumor with microscopically negative margins showing no evidence of tumor cells (sometimes called "clean" margins).
- R1 resection indicates that the margins of the resected parts show tumor cells when viewed microscopically – microscopically positive margins.
- R2 resection indicates that portions of tumor visible to the naked eye were not removed -macroscopically positive margins.
In a surgical resection, the cut edge of the specimen is marked with ink (often black or blue in color) and the areas that are closest to the tumor are carefully examined under the microscope. If the tumor is touching ink, then it is possible that there is tumor still present in the patient, and this is considered a "positive" margin. The outer serosal surface of the stomach or bowel is not a true margin, because it does not connect to an adjacent structure, but reports will sometimes mention if tumor penetrates the serosal surface as this may have implications for seeding of the peritoneal (abdominal) cavity.
Microscopic Description: Morphology and Histology
Morphology refers to the characteristics of individual cells, and histology refers to the description of the microscopic structure of tissues. You could think of tissue structure as similar to the grain of wood. The pathologist will comment on the overall organization of the tumor cells as viewed on prepared slides, as well as features of individual cells.
For these observations, the pathologist usually uses H&E slides (slides stained with hematoxylin and eosin). Hematoxylin stains cell nuclei blue, and eosin stains other cell parts pink. Using H&E is standard to help the pathologist view cells better. Your report may contain the word "eosinophilic" which simply indicates how much the cells took up the eosin stain. If they stained dark pink with eosin the description might be "brightly eosinophilic" and if they stained only a little the description might be "palely eosinophilic." This is simply descriptive and is not important for GIST prognosis.
Cellularity: Your report may comment on "high cellularity" if the tumor cells are densely packed, or "low cellularity" if they are not so crowded, and if there are non-tumor supporting cells (called stroma) in between sections of tumor cells. High cellularity might indicate that the tumor cells have been actively dividing more rapidly, but it is the assessment of the mitotic rate that is most predictive of behavior.
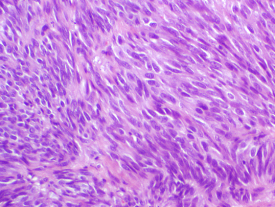
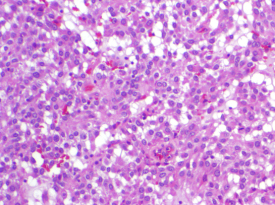
Cell types in GIST: The pathologist will describe the GIST cells’ shape as spindle, epithelioid, or mixed. Overall, about 70% of GISTs are composed of spindle cells (long and skinny in shape, sometimes called fusiform), while 20% are composed of epithelioid cells (round or polygonal), and 10% contain a mixture of both types. However, the cell shape distribution does vary among GISTs from different digestive tract organs. Almost all intestinal GISTs are of the spindle cell type, but about 40% of gastric GISTs (arising from the stomach) show epithelioid morphology or mixed cell type. Epithelioid GISTs are more likely to be PDGFRA-mutant or to be wild-type than spindle cell GISTs. Both cell types are shown in Figure 4.
 |
 |
|
Spindle cell GIST stained with hematoxylin and eosin. |
Epithelioid cell GIST stained with hematoxylin and eosin. |
|
Figure 4. Spindle cell and epithelioid cell GIST viewed at 100X magnification. |
|
Other cell characteristics: The pathologist may note various other cell features that are not typical of normal cells. In general, in sarcoma grading, the more similar the tumor cells appear to normal cells, the more favorable the outcome may be. However, in GIST this relationship does not clearly hold true. Nonetheless, the following terms might appear in your report:
- Nuclear atypia: abnormal appearance of the nucleus of a cell.
- Pleomorphism: lack of uniformity in cell appearance, extreme variation in cell shape and size (including nuclear variation); this is uncommon in GIST.
Tissue structure characteristics: Your report may mention patterns in the structure of the tissue (whorls, fascicles, palisades, sheets, nests, etc.), but this is of little significance in terms of prognosis.
Serosal penetration: If the tumor is quite small and is still contained within the wall of the GI tract, it is called "intramural." Sometimes larger tumors will grow outward through the wall of the digestive organ where it originated, and penetrate the serosal membrane covering the muscular wall. Penetration of the serosa may be associated with an increased risk of metastasis within the abdominal cavity, but this is not one of the critical features for prognosis.
Tumor vascularity (blood supply): The pathologist may note how richly the tumor was served by blood vessels. Tumors cannot grow very large without developing new vessels to bring them blood. Most GISTs are highly vascular.
Mitotic count or Mitotic rate
Mitosis means cell division, the process by which cells proliferate or reproduce. Tumors grow because the tumor cells divide too frequently. The more often each cell divides, the faster the tumor grows. The mitotic count is one of the most important parts of your pathology report because this proliferation indicator helps predict the probability that surgery was curative versus the probability that GIST might recur.
Here is a figure illustrating the steps in the cell division cycle. Mitosis is the final step, when the cell actually separates into two. The pathologist can see how many cells are in the division process when examining slides of tumor cells under the microscope.

Figure 5. The cell cycle.
The cell cycle consists of two growth phases, G1 and G2, that separate the synthetic (DNA replication) and mitotic (cell division) phases. After mitosis, cells can enter the G0 resting phase for a variable amount of time. Under stimulation from a constitutively active KIT receptor, the time that GIST cells spend in G0 is greatly reduced.
The mitotic count is one of the most important parts of your pathology report because it indicates how fast your GIST was growing. Higher mitotic rates strongly suggest an increased chance that the tumor will recur in the future, as detailed in the section on prognosis.
To determine mitotic rate, the pathologist literally counts the number of cells that can be seen undergoing mitosis (called mitotic figures) in a specified section of the tumor. Different parts of the tumor may be growing more actively than others, so the pathologist should carefully evaluate different sections and perform the count on the section with the highest mitotic rate they can find. Once that most actively growing section has been identified, the pathologist will examine 50 consecutive high-power fields (50 HPF) under the microscope to count mitoses.
One high-power field is a standard measure of area, and 50 traditional HPF equals 5 square millimeters (5 mm2). If the pathologist uses a microscope with fields twice as big (called wide-field optics) then only 25 fields are needed to contain the same area of 5 square millimeters (5 mm2). The count will be reported as a ratio such as 3 / 50 HPF (3 mitoses per 50 HPF) or 15 / 50HPF (15 mitoses per 50 HPF). Values less than 5 / 50 HPF are desirable, and values over 20 / 50 HPF are exceptionally high.

Figure 6. GIST cells at 400X magnification with mitotic figures circled, illustrating what the pathologist looks for to count the mitotic rate.
Some pathologists also use an alternative indicator of tumor cell division called Ki-67 or MIB-1. This is an immunohistochemical stain that identifies cells in any non-resting stage of the cell cycle (anything but G0). The result is given as the percent of cells that have entered the cell cycle. This method and mitotic counts are similar in assessing cell proliferation, but the two do not easily translate one to the other, and extensive studies to validate the prognostic value of specific levels of nuclear MIB-1 reactivity have not been performed in GIST.
Immunohistochemical Tests
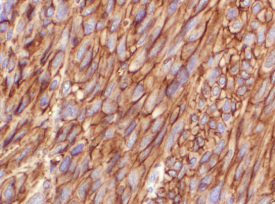
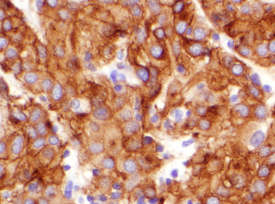
Immunohistochemical tests use antibodies to detect whether selected proteins are present in cells. All cells have many parts composed of proteins, but cells of different types (such as muscle cells versus nerve cells versus bone cells) use different specific proteins for their particular cell functions. Antibodies can be prepared that will bind to the protein of interest in a sample of tumor cells. In this context, the protein being tested for is called an antigen. Binding of the antibody to the antigen forms a new target that can be stained to show its presence in the cells. Multiple steps are usually involved in performing immunohistochemical tests, but at the end the pathologist knows whether the tumor cells stain for the proteins that were tested for. Positive results for KIT are illustrated in Figure 7.
 |
 |
|
KIT-positive spindle cell GIST. |
KIT-positive epithelioid cell GIST. |
|
Figure 7. Spindle cell and epithelioid cell GIST viewed at 200X magnification with brown staining indicating positive results for KIT immunohi |
|
Although staining for KIT protein (CD117) is usually diagnostic for GIST, the pathologist often performs other tests as well to rule out competing diagnoses. The histologic appearance of the tumor, along with its location, suggests a few alternative tumor types to the pathologist, who selects a panel of tests to identify the correct diagnosis. A typical test panel might include the following immunohistochemical tests. They have no prognostic significance for GIST but are done to aid in differential diagnosis.
- CD34 This test is positive in about 80% of gastric GISTs but only about 50% of intestinal GISTs.
- SMA or smooth muscle actin is positive in about 30% of GISTs.
- S100 is positive in about 5% of GISTs.
- Desmin is positive in about 2% of GISTs, most commonly in GISTs that are negative for KIT.
- Pan-keratin is positive in <1% of GISTs.
The main competing diagnoses for abdominal tumors are listed in the following table, along with the immunohistochemical tests that indicate each one.
| Cell shape | Tumor Type | Examples | Characteristic Immunohistochemistry |
| Spindle |
Smooth muscle tumors | Leiomyoma Leiomyosarcoma |
smooth muscle actin + desmin + |
| Neural tumors | Schwannoma Malignant peripheral nerve sheath tumor |
S-100 protein + | |
| Fibrous tumors | Inflammatory fibroid polyp Solitary fibrous tumor |
CD34 + | |
| Desmoid fibromatosis | smooth muscle actin + beta-catenin (nuclear) + |
||
| Carcinoma | Spindle cell carcinoma | pan-cytokeratin + | |
| Epithelioid |
Melanoma | Melanoma | melan-A + HMB45 + S-100 protein + |
| Perivascular tumor | PEComa (perivascular epithelioid cell tumor) |
smooth muscle actin + HMB45 + |
|
| Carcinoma | Clear cell carcinoma | pan-cytokeratin + |
KIT protein (CD117) is important for GIST diagnosis, but other markers such as DOG1 and CD34 can also be useful. Tumors other than GIST may also show some staining for KIT. Therefore, additional immunohistochemical tests selected by the pathologist are used to evaluate the competing diagnoses.
KIT-negative GISTs also exist. About 5% of GISTs do not test positive for KIT (CD117). This group includes some (but not all) GISTs with mutations in the gene for PDGFRA, as well as some GISTs with mutations in the KIT gene, and some GISTs with neither mutation (wild-type). The immunohistochemical tests that can sometimes help to identify KIT-negative tumors as GIST include the following:
- DOG1 – a marker that may be positive in KIT-negative GISTs (about 40%)
- PDGFRA – the growth factor receptor positive in GISTs with mutations in the gene for PDGFRA, but the available immunohistochemical tests are not widely used due to reliability issues
Diagnosis
Once the pathologist has described all the tests required for the individual case, the pathologist will state the diagnosis of GIST and often give a brief rationale for this conclusion. Some pathology departments use the term "gastrointestinal stromal sarcoma" (as opposed to gastrointestinal stromal tumor) for tumors that have greater malignant potential.