

Surgery for Metastatic GIST
Frequently, gastrointestinal stromal tumor (GIST cancer) is already metastatic at the time of diagnosis. GIST metastases typically involve the liver and/or the peritoneum. In this case the surgeon may not be able to resect all visible tumors. If feasible, resection is advisable, even though surgery for metastatic GIST is not potentially curative, as some GIST cells are certain to remain post-surgery. Therefore, adjuvant imatinib (Gleevec) is the standard of care to attempt to prevent further recurrences.
Surgery for GIST metastases that have been downsized by imatinib or sunitinib therapy has been reported with good results if the resection is done while the tumors are still under control (before drug resistance) and if drug therapy is continued post-surgery. One rationale for resecting metastases is to eliminate tumors from which drug-resistant clones might develop. Several eminent GIST surgeons advocate resection of metastatic GIST within one year of starting imatinib (Gleevec) therapy, in order to prevent potential development of drug resistance (Gold and DeMatteo, 2006; Raut and Ashley, 2008).
Raut et al (2005 CTOS presentation; Raut et al, 2006) compared progression-free survival and overall survival for three groups of patients who had surgery after a period of imatinib or sunitinib therapy:
- stable disease (initially unresectable cases in which drug therapy had shrunk tumors to a potentially resectable state, and all tumors were stable prior to surgery)
- limited progression of disease (initially unesectable cases for whom drug therapy did not render all tumors resectable, with progression of one or more areas of disease while other areas remained under drug control, and the progressing areas had a chance to be completely resected)
- generalized progression (unresectable cases for whom multiple areas of disease showed progression, and surgeons determined that the progressing areas could not be completely resected, but debulking could be done).
Figure 1 from Raut et al (2006) shows the course of GIST after surgery for these three groups of patients. Note that only 78% of the stable-disease group, 25% of the limited-progression group, and 7% o the general-progression group achieved “no evidence of disease” status following surgery. The majority of patients (about 60%) with stable disease retained progression-free status 20 months post-surgery, compared to about 20% of patients with limited progression. However, patients with generalized progression quickly showed additional progression after debulking surgery.
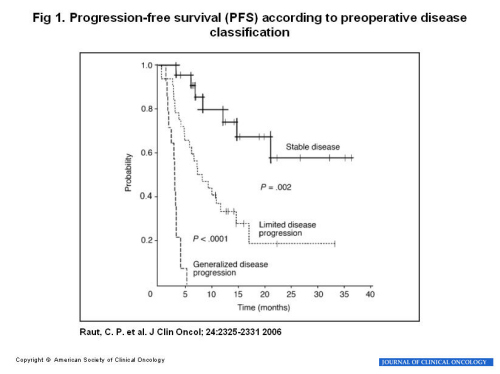
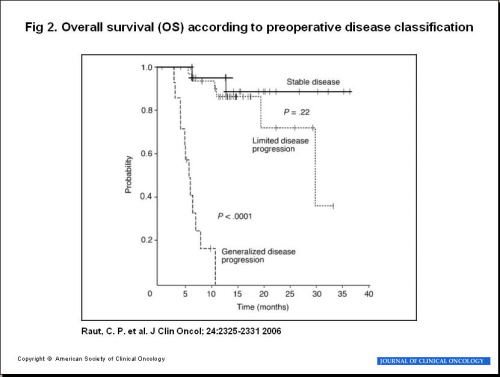
Figure 2 from Raut et al (2006) shows corresponding data for overall survival. The group with stable disease prior to surgery showed longer survival after surgery than did the group with limited progression. Although the study did not permit any quantification of how much surgery contributed to lengthening progression-free survival and overall survival, the authors concluded that surgery is worthwhile if all tumor can be removed during a period of stability. Surgery probably adds to progression-free and overall survival time if done during limited progression. Surgery’s benefit is limited to symptom reduction if there is generalized progression. The authors urged that prospective trials be undertaken to quantify these benefits. The authors stated “In conclusion, patients presenting with stable advanced GISTs on KIT-directed therapy experienced prolonged PFS (progression-free survival) and OS (overall survival) after surgery. Those with limited disease progression usually progressed within 12 months of surgery, but appear to have an improved OS.”
Additional small series of patients who underwent surgery while their metastatic GIST tumors were responding to tyrosine kinase inhibitors (TKIs) imatinib or sunitinib have reported similar results. Data from several such studies are summarized in the following table for patients whose surgeries were performed prior to the development of drug resistance. (Note that patients with neoadjuvant treatment of primary tumors are not included in this table.) Recurrences following surgery appear related to these factors:
- whether complete resection can be achieved
- whether the patient resumes TKI drug therapy after surgery.
|
Recurrences after surgery in patients while stably responding to imatinib or sunitinib tyrosine kinase inhibitors (TKIs). |
|||
| Source | Number Patients |
Recurrences With TKI Drugs Continued |
Recurrences Without TKI Drugs |
| Bauer et al (2005) | 12 | 1 of 10 (10%) | 1 of 2 (50%) |
| Gronchi et al(2007) | 27 | 4 of 24 (17%) | 2 of 3 (67%) |
| DeMatteo et al (2007) | 20 | 3 of 16 (19%) Patients with recurrence had R2 resections. |
4 of 4 (100%) |
| Rutkowski et al (2006) | 19 | 1 of 19 (5%) | not applicable |
| Sym et al (2008) | 16 | 0 of 6 (0%) | 7 of 10 (70%) |
Surgery for Drug-Resistant Tumors
During imatinib (Gleevec) treatment, a patient’s tumor(s) may be under control for a prolonged period, followed by the emergence of an area of new growth inside of an otherwise controlled tumor. This phenomenon has been referred to as a “nodule within a mass” or as “partial resistance” or “focal resistance.” For liver metastases, radio frequency ablation of the growing area has been used. The patient then continues on imatinib therapy for the tumors still under drug control.
Another type of focal resistance occurs in patients with several metastases in the peritoneum or mesentery when one such tumor becomes resistent to imatinib and resumes growing. Surgical resection has been used to remove the resistant tumor. Sometimes it is possible to remove all visible metastases, but more often there are still residual unresectable tumors left after resection of the resistant tumor. Several surgical reports have described the results of resection in the case of focal progression (R
utkowski et al, 2006; Gronchi et al, 2007; DeMatteo et al, 2007; Hasegawa et al, 2007; Sym et al, 2008). The benefit of this surgery is uncertain. Most patients show progression of remaining (previously stable) tumors within 3-12 months. Benefit may be greater in cases where all visible disease can be removed.
Also see the graphs and discussion above regarding the limited-progression group in the study of Raut et al (2005, 2006).
In the case of generalized progression (most or all tumors growing in spite of drug therapy), the results of all available studies indicate no benefit except to make the patient more comfortable. Rapid recurrence within 3 months was found in such cases by the following investigators: Rutkowski et al (2006), DeMatteo et al (2007), and Sym et al (2008).
REFERENCES
Andtbacka RH, Ng CS, Scaife CL, Cormier JN, Hunt KK, Pisters PW, Pollock RE, Benjamin RS, Burgess MA, Chen LL, Trent J, Patel SR, Raymond K, Feig BW.
Surgical resection of gastrointestinal stromal tumors after treatment with imatinib.
Ann Surg Oncol. 2007 Jan;14(1):14-24.
PMID: 17072676
Bauer S, Hartmann JT, de Wit M, Lang H, Grabellus F, Antoch G, Niebel W, Erhard J, Ebeling P, Zeth M, Taeger G, Seeber S, Flasshove M, Schutte J.
Resection of residual disease in patients with metastatic gastrointestinal stromal tumors responding to treatment with imatinib.
Int J Cancer. 2005 Nov 1;117(2):316-25. PMID: 15900603
DeMatteo RP, Maki RG, Singer S, Gonen M, Brennan MF, Antonescu CR.
Results of tyrosine kinase inhibitor therapy followed by surgical resection for metastatic gastrointestinal stromal tumor.
Ann Surg. 2007 Mar;245(3):347-52. PMID: 17435539
Gold JS, Dematteo RP.
Combined surgical and molecular therapy: the gastrointestinal stromal tumor model.
Ann Surg. 2006 Aug;244(2):176-84. Review.
PMID: 16858179 Free access in PubMed
Gronchi A, Fiore M, Miselli F, Lagonigro MS, Coco P, Messina A, Pilotti S, Casali PG.
Surgery of residual disease following molecular-targeted therapy with imatinib mesylate in advanced/metastatic GIST.
Ann Surg. 2007 Mar;245(3):341-6. PMID: 17435538
NCCN, National Comprehensive Cancer Network.
Soft Tissue Sarcoma Guidelines
Raut CP, Posner M, Desai J, Morgan JA, George S, Zahrieh D, Fletcher CD, Demetri GD, Bertagnolli MM.
Surgical management of advanced gastrointestinal stromal tumors after treatment with targeted systemic therapy using kinase inhibitors.
J Clin Oncol. 2006 May 20;24(15):2325-31.
PMID: 16710031
Raut CP, Ashley SW.
How I do it: surgical management of gastrointestinal stromal tumors.
J Gastrointest Surg. 2008 Sep;12(9):1592-9.
PMID: 18317848
Raut CP, Desai J, Morgan JA, George S, Posner M, Zahrieh D, Fletcher CDM, Demetri GD, Bertagnolli MM.
Surgical management of advanced GIST following KIT-directed therapy.
Slide show from presentation at 2005 meeting of Connective Tissue Oncology Society.
Rutkowski P, Nowecki Z, Nyckowski P, Dziewirski W, Grzesiakowska U,Nasierowska-Guttmejer A, Krawczyk M, Ruka W.
Surgical treatment of patients with initially inoperable and/or metastatic gastrointestinal stromal tumors (GIST) during therapy with imatinib mesylate.
J Surg Oncol. 2006 Mar 15;93(4):304-11. PMID: 16496358
Scaife CL, Hunt KK, Patel SR, Benjamin RS, Burgess MA, Chen LL, Trent J, Raymond AK, Cormier JN, Pisters PW, Pollock RE, Feig BW.
Is there a role for surgery in patients with “unresectable” cKIT+ gastrointestinal stromal tumors treated with imatinib mesylate?
Am J Surg. 2003 Dec;186(6):665-9.
PMID: 14672776
Sym SJ, Ryu MH, Lee JL, Chang HM, Kim TW, Kim HC, Kim KH, Yook JH, Kim BS, Kang YK.
Surgical intervention following imatinib treatment in patients with advanced gastrointestinal stromal tumors (GISTs).
J Surg Oncol. 2008 Jul 1;98(1):27-33. PMID: 18452195