

Nomogram for Estimating the Probability of Recurrence-Free Survival after Surgical Resection of Primary GIST
 GIST Support International posed questions about predicting the probability of curative surgery to Ronald P. DeMatteo, MD FACS.
GIST Support International posed questions about predicting the probability of curative surgery to Ronald P. DeMatteo, MD FACS.
Dr. DeMatteo is Vice Chair of the Department of Surgery, as well as Head of the Division of General Surgical Oncology at Memorial Sloan-Kettering Cancer Center in New York City. In 2009 he was named to the Leslie H. Blumgart Chair in Surgery. Dr. DeMatteo is known internationally as an expert in GIST surgery, and he has been one of the prime movers behind several GIST trials. Currently he is the principal investigator of the Z9001 trial and the NCT00867113 trial evaluating adjuvant Gleevec. Dr. DeMatteo is active in the NCCN Task Force on GIST. He is the principal co-author of the book 100 Questions & Answers About Gastrointestinal Stromal Tumor (GIST). His research includes developing immune therapies to help prevent tumors from returning after surgery. You can read more about him at his webpage and you can read an interview with him at the MSKCC website. Over the years many GIST patients have expessed their appreciation of Dr. DeMatteo’s gentlemanly demeanor and his kind and respectful bedside manner.
Recently Dr. DeMatteo and colleagues published a paper describing a nomogram to estimate the probability of recurrence-free survival after surgery for a primary GIST. Here is the citation, and you can link to the PubMed abstract.
Gold JS, Gönen M, Gutiérrez A, Broto JM, García-del-Muro X, Smyrk TC, Maki RG,Singer S, Brennan MF, Antonescu CR, Donohue JH, DeMatteo RP.
Development and validation of a prognostic nomogram for recurrence-free survival after complete surgical resection of localised primary gastrointestinal stromal tumour: a retrospective analysis.
Lancet Oncol. 2009 Nov;10(11):1045-52. PubMed PMID: 19793678
This nomogram should be useful to GIST patients in considering their treatment options, so we asked for more information about it.
Below are Dr. DeMatteo’s responses to GSI’s questions.
1. What is a nomogram?
A nomogram is a mathematical model that can be used to estimate the likely outcome for a given patient. The GIST nomogram is available in a calculator version on the MSKCC website .
2. Please explain the variables in the GIST nomogram.
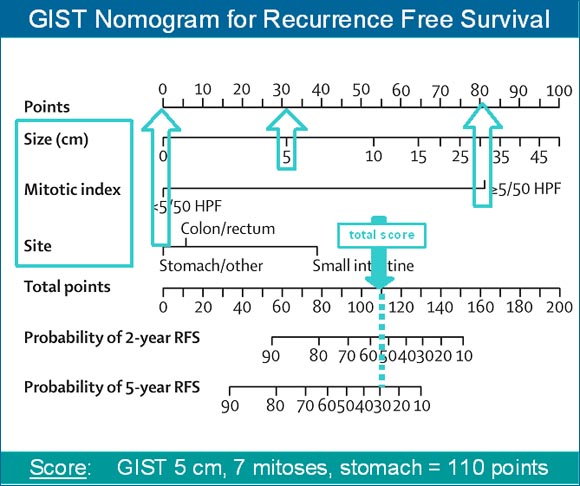
The nomogram is based on tumor size in centimeters, the location of the tumor, and the mitotic rate. Mitotic rate is determined by a pathologist. The higher the mitotic rate, the more actively dividing a tumor’s cells appear under the microscrope.
![]()
Reprinted from The Lancet Oncology, Vol. 10 number 11, Gold et al, Development and validation of a prognostic nomogram for recurrence-free survival after complete surgical resection of localised primary gastrointestinal stromal tumour: a retrospective analysis, Copyright 2009, with permission from Elsevier.
3. What are the purposes for which this GIST nomogram might be used?
It may be used to estimate the likelihood of tumor recurrence in a given patient. Therefore, it also may be used to select patients for adjuvant therapy. It must be emphasized that what will happen in any given patient cannot be determined. The nomogram is just a general guide to what is likely to occur.
4. How might this help a patient decide whether to take adjuvant imatinib?
If a patient is at high risk of recurrence, then the physician and doctor may decide that adjuvant imatinib should be administered. Conversely, if the risk of recurrence is very low, then the decision may be just to undergo observation and not take adjuvant therapy.
5. Can you show an example to illustrate how to use the nomogram to calculate the probability of recurrence-free survival at 2 years and at 5 years?
In this particular example shown below, a patient has a 5 cm stomach tumor with a high mitotic rate. Read upwards for each variable to get the individual points (30 points for size, 80 points for mitotic index, 0 points for site). Then add the 3 point values together to get the total points (110 total points). From total points, read downward to get the 2- and 5-year likelihood of recurrence-free survival. In this example the probability of recurrence-free survival at 2 years is about 55%, and at 5 years it is about 30%. Conversely, the risk of recurrence at 2 years is about 45% (100% – 55%) and at 5 years it is about 70% (100% – 30%).
6. Some critics have pointed out that when using the nomogram, a difference in mitotic rate from 4/50 to 5/50 causes a huge jump in the predicted risk of recurrence. This same criticism has been made of the Miettinen and Lasota / AFIP risk scheme. Do you have plans to further refine the mitotic rate into 3 or 4 categories (such as <5, 5-10, 10-20, and >20)? Do you think there is a greater probability of recurrence for a patient with a mitotic rate of 25/50 HPF than for a similar patient with a rate of 7/50 HPF?
Yes, we will further refine the model at some point. Nevertheless, a cutoff of 5 mitoses has proven to be very reliable overall in several studies.
7. Would information about tumor rupture (whether spontaneous or spillage during resection)further refine the risk of recurrence? Do all types of ruptures equally increase risk of recurrence?
We believe that rupture does increase the risk of recurrence. We did not have enough patients in the populations that we studied to include it in the nomogram. We do not know if there is a difference between preoperative and intraoperative tumor rupture.
8. We know that GIST can recur after 10 or even 20 years, but this is rare, and most recurrences happen within 3 years of resection. The median years of followup in the 3 datasets assessed with the nomogram were 3-5 years. Do the data upon which the nomogram was validated have enough years of follow-up to find the vast majority of recurrences? Do you have plans to obtain more years of follow-up for your 3 datasets?
Some patients do develop tumor recurrence after 5 years and in some it can even take 10 years. Adjuvant imatinib may delay recurrence. So we need longer follow up to improve our ability to estimate recurrence.
9. Are there plans to use the nomogram on data from the Z9000 or Z9001 trials? If so, please describe.
Yes, the nomogram will be applied to the national GIST trials.